60yrs /F with Pain in chest , breathlessness,and fever
Welcome and greetings to every one who are visiting my blog. This is an online E log platform to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. I have been given this case in order to solve in an attempt to understand the topic of patient's clinical data analysis to develop my competency in reading and comprehending clinical data and come up with a diagnosis and treatment plan.
25/11/22
CHEIF COMPLAINT
60yrs /F farmer by occupation came to OPD with c/o Pain in chest , breathlessness,and fever on 26/11/22
HOPI(History of present illness):
Patient was apparently asymptomatic 4 days back
Then day she developed breathlessness gradually progreessed from mMRC grade 2-3
History of fever 2days
And there is history of Vomitings and nausea ,fever,
history of chest pain 2 days dragging pain
PAST HISTORY:
a K/c/o HTN for 1 yrr on treatment medication T.Aten 50 mg OD
T.Amlodepine 5 mg OD
Not a K/c/o DM, BA , Thyroid disorder and Epilepsy.
Hysterectomy -18 yrs back
PERSONAL HISTORY:
Married
Occupation -Farmer
Diet - mixed
Appetite - normal
Sleep - adequate
Bowel and bladder movements - regular
She have habit of drinking toddy and stoped before 1 year
No habit of betel nut, beatel leaf
FAMILY HISTORY:
No similar history in the family
Obse
GENERAL EXAMINATION:
-Patient is conscious,coherent and cooperative at the time of joining
-No pallor
-No icterus
-No lymphadenopathy
-No cyanosis
-No clubbing of fingers
-No edema of feet
-No malnutrition
-No dehydration
▪️VITALS:
Temperature - 99F
Pulse rate - 98 bpm
Respiration rate - 32cpm
BP - 140/70 mmhg
SpO2 - 84% @ RA at 95% 6lit of O2
GRBS-236mg %
SYSTEMIC EXAMINATION:
▪️CVS
-no thrills
-no cardiac murmurs
S1&S2 sounds are heard
▪️RESPIRATORY SYSTEM
Upper respiratory tract
Nose no DNS polyps tuburinate hypertropy
Oral cavity poor oral hygiene
Posterior Pharyngeal wall
Lower respiratory tract
Shape of the chest bilaterally symmetrical elliptical
Trachea appear to be central
Supra clavicular and infra clavicular Hollowness
Crowding of ribs and dropping of shoulder absent
Muscles wasting- absent
Apical impulse -not seen
Kyphoscoliosis- absent
Scars and pigmentation -absent
Palpation
All inspestory findings are confirmed
No local rise in temperature
Trachea central
Apex beat. 5th intercoastal space along the mid clavicular line
Percussion
Direct -resonant
Indirect - dull. In left infra axillary area
Interscapular area and interscapular area
Right. Left
Supra clavicular. R. R
Infra clavicular R. R
Infra axillary. R. Dull
Suprascapular . R. R.
Interscapular. R. Dull
Infrascapullar. R. Dull
Ascultation
Crepts are heard
Vesicular beath sounds
▪️CNS
No nerological defect
Provisional diagnosis
Bilateral lung consolidation secondary to
Investigation
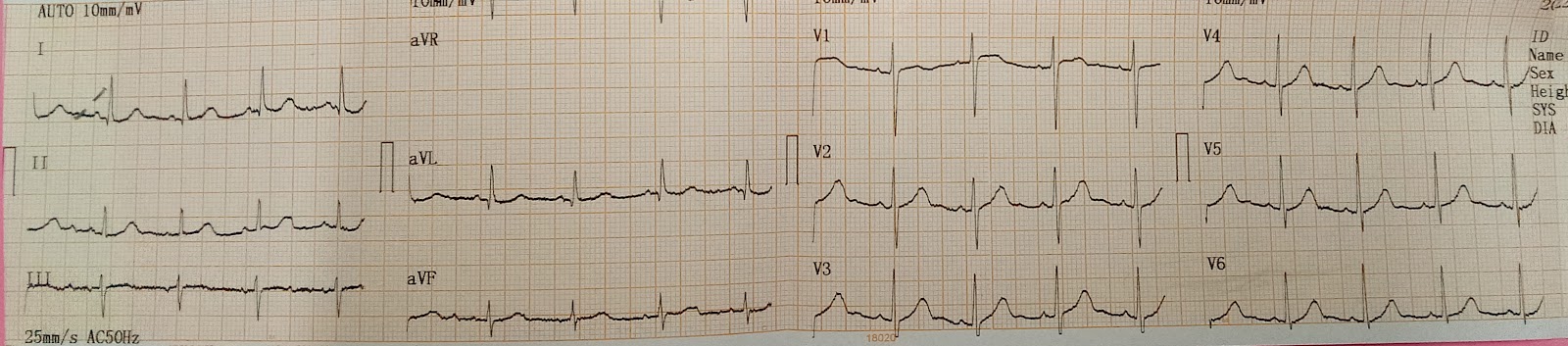
ECG
2D echo
Blood count
Rft and Lft

Treatment
O2 inhaltion through face mask
Inj. Agumentin 1.2gm/i.v/TID


